导图社区 SDU人体PBL4
- 31
- 0
- 0
- 举报
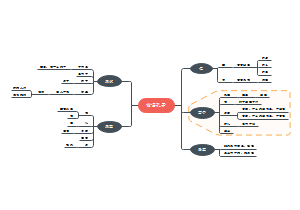
SDU人体PBL4
关于SDU人体PBL4的思维导图,整理了SYMPTOMS、ASSUMPTION、CLUES-1、CLUES-2、CLUES-3、DIAGNOSIS、TREATMENT的内容,希望这份脑图会对你有所帮助。
编辑于2023-03-18 23:16:51 山东省- 框图
- 相似推荐
- 大纲

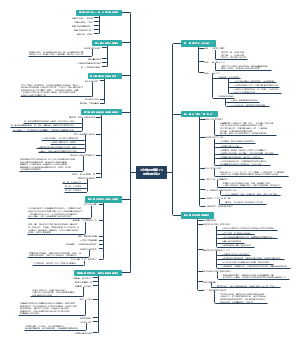

AFTER PICNIC
SYMPTOMS
Patient is female, 17 years old, previously healthy. Abdominal pain, chest tightness and nausea occurred 3 hours after consumption of unknown species of white mushroom. Chest tightness and abdominal pain worsened 7 hours later, so Starasol was self-administered. 9 hours later, she looked pale, sweating and vomiting. She arrived at the hospital with cold limbs, shortness of breath, lethargy and unconsciousness.
T 37°C,HR 110 per min R 30 per min,BP 85/55mmHg
ASSUMPTION
Food poisoning acidosis? sympathetic shock?
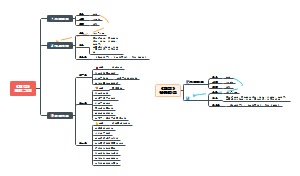
CLUES-1
SCr 200umol/L→260umol/L Ccr 60ml/min→40ml/min
serum creatinine(Scr)
clinical significance
Creatinine : 1. end product of muscle creatine metabolism 2.used in clinical setting to measure GFR but less accurate 3.small amount secrete from the tubule
physiologic 1.exercise level, diet, age 2.reduced: the elderly, malnutrition
acute kidney injury, AKI
1. The main basis of diagnosis
2. Clinical stage
3. Differential diagnosis of prerenal and renal oliguria
Conclusion : organic oliguria and improved after treatment.
The patient was in the stage of azotemia.
endogenous creatinine clearance rate (Ccr)
clinical significance
computational formula
Early diagnosis of glomerular injury
1.exercise level, diet, age
2. Pathological decrease
Sensitive to renal impairment
case : 60ml/min
Chronic kidney disease (CKD)
1. Diagnostic basis :Ccr<60ml/min, for >3mo
2. Clinical stage
case : drop to 40ml/min and improve to 70ml/min after treatment
Conclusion: Glomerular filtration function was moderately impaired and gradually returned to normal.
CLUES-2
BUN 20mmol/L→30mmol/L
Nitrogen-containing metabolic wastes (urea, creatinine, uric acid, etc.), urea accounts for 80%~90%.
source
Urea cycle
excretion: Glomerular filtration or Transport of renal tubules
function
Participate in the formation of intramedullary osmotic pressure gradient Rough observation of glomerular filtration function Differential diagnosis of upper and lower gastrointestinal bleeding Uremic toxin
Urea and its catabolic metabolite cyanate can cause some uremic symptoms, such as anorexia, nausea, vomiting, diarrhea, bleeding tendency, impaired glucose tolerance, hypothermia and coma, etc. Cyanate can cause carbamylation of proteins and amino acids, affecting its normal function.
case:Scr 200mmol/L → 260mmol/L →180mmol/L
proteinuria(+++),there is RBC,WBC and granule tube type in urine
urinalysis
proteinuria(+++)
Physiological proteinuria:functional or postual
Pathological proteinuria
Urine microscopy
Urinary red blood cells Increased number of red blood cells in centrifuged urine, exceeding 3/HPF
Urinary leukocytes Mainly used for diagnosis of urinary system infection Increased number of white blood cells, exceeding 5/HPF Pyelonephritis, cystitis, renal transplant rejection, drug-induced acute interstitial nephritis, crescent glomerulonephritis, poisoning, vaginitis, and cervicitis
Cast is a cylindrical protein aggregate formed by coagulation of proteins, cells, and their disintegrating products in renal tubules and collecting ducts, and is the most diagnostic component of urinary sediment.
Conditions
Granular cast
CLUES-3
Amanita fatalisc(white mushroom)
Characters: The meat is large, distributed widely in the middle and south of our country
Toxigenic substances: toxigenic peptides: amanita toxigenic peptides (the main toxigenic substances), ghost toxigenic peptides; Amanita peptide: alpha-amanita carinic acid
Clinical symptoms: initial: nausea, vomiting, abdominal pain, diarrhea; Middle stage: dyspnea, restlessness, whispering; Facial muscle spasm, calf muscle spasm; Late stage: liver and kidney damage, especially liver damage is the most serious and dangerous
Toxogenic mechanism: Toxopeptides and toxopeptides can specifically inhibit true and cellular RNA polymerase, prevent mRNA elongation, and induce cell apoptosis
Treatment: drug expulsion therapy and drug antidotes. Drug expulsion treatment includes gastric lavage; Activated carbon therapy; Diarrhea, bile drainage, in vitro elimination (including hemodialysis, hemoperfusion, molecular adsorption recirculation system, graded plasma separation and adsorption), antidotes include: penicillin G, ceftazidime, n-acetylcysteine; Silymarin and ganoderma lucidum decoction. But there is a lack of specific drugs
Future direction: research and development of anti-tumor drugs; Biological control of pests and animals
DIAGNOSIS
Food poisoning, shock, acute kidney injury with hyperazotemia, hyperkalemia, metabolic acidosis due to consumption of amanita fatally
Grade of renal insufficiency
AKI
Diagnostic criteria: Serum creatinine increased by 0.3mg/dl (≥26.5μmol/L) within 48h. Renal impairment was known or assumed to occur within 7 days, and serum creatinine rose to > 1.5 times the baseline value (44-133μmol/L) Urine volume < 0.5ml/ (kg·h) for 6h
Chronic renal failure
Diagnostic criteria: Renal injury ≥3 months, albuminuria, abnormal urinary sediment, tubular related lesions, histological abnormalities, radiological structural abnormalities, any of the kidney transplant history GRF < 60ml/ (min·1.73m^2) for 3 months
Stage of AKI
Oliguric AKI
Oliguria stage Oliguria or anuria; There were protein, RBC, WBC and hyaline tube in urine. Water poisoning; Hyperazotemia; Hyperkalemia; Metabolic acidosis It lasts 7-14 days, up to a month for the elderly. The longer this period, the worse the prognosis.
Polyuria stage Urine volume reached 400mL/d because GFR was restored but tubule reabsorption was not fully restored, the retained nitrogenous metabolic waste was osmotic diuretic, and the protein tubule blockage was relieved. Hyperazotemia and hyperkalemia were still present in the previous week, and the patient remained in critical condition. Loss of water and electrolytes after a week may lead to dehydration, hyponatremia, hypokalemia, and susceptibility to infection. It lasts 2 weeks
Convalescence period Blood biochemical indexes returned to normal, however, it took about six months to one year for renal tubule reabsorption function to fully recover.
Non-oliguric AKI Cause: Some people think that the damage of GFR is not serious; Acute kidney injury caused by aminoglycoside antibiotics is mostly of this type; Prompt intervention and effective drug use have increased the rate of such AKI in recent years. The urine volume was more than 400mL/d, and there was hyperazotemia Clinically, it is often ignored due to normal urine volume and may develop into oliguric AKI without timely intervention. Oliguric AKI can be transformed into non-oliguric AKI by appropriate and timely intervention.
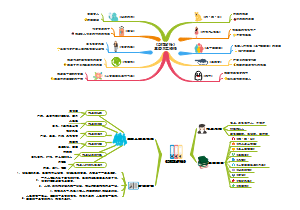
TREATMENT
Gavage, ECG monitoring, fluid replenishment, oxygen inhalation (to expel toxins, prevent cardiac arrest caused by hyperkalemia, replenish blood volume to correct shock). After diagnosis of AKI, intravenous infusion of 20% mannitol, furosemide, 25% glucose plus insulin was given (to correct hyperkalemia), and NaHCO3 was given (to correct metabolic acidosis). Hemodialysis was performed after diuretic effect was found to be unsatisfactory. After 22 days, hypokalemia was found in the polyuria stage, and KCl was given orally.
Hematodialysis: The patient's blood and dialysate are injected into the dialyzer at the same time. The semi-permeable membrane diffusion of the dialyzer is used to remove small molecular metabolic wastes or harmful substances in the blood
gastric lavage: It refers to pouring a certain amount of liquid into the stomach cavity, mixing the contents of the stomach, and then extracting it. Repeat this process for many times. Its purpose is to clear the unabsorbed poison in the stomach or clean the stomach cavity
AKI treatment
AKI progonosis
Death rate
without complications:7%~23% with complications:50%~80%
Resume:It takes 0.5 to 1 year for the damaged renal cell function and structure to fully return to normal
Treatment of oliguria
Correct water electrolyte disorders
Maintain fluid balance (1)Measure out as in Treatment of hyperkalemia (1)Dialysis therapy (2)Intravenous calcium gluconate (3)Intravenous glucose plus insulin (4)Diuretics Treatment of hyponatremia (1)Control moisture Treatment of hypocalcemia (1)Inrevenous calcium gluconate Treatment of hyperphosphatemia (1)Limit phosphorus intake
Correct acidosis
Pay attention to diet and nutrition
Prevention of infection
Free radical scavenger Calcium channel antagonist ACEI PGI2 or PGE2
Blood essence therapy
Treatment of polyuria
Maintain water electrolyte and acid-base balance
Control azotemia
Treatment of primary diseases and various complications
Convalescent treatment
No special treatment required