导图社区 Immune system
- 29
- 0
- 0
- 举报
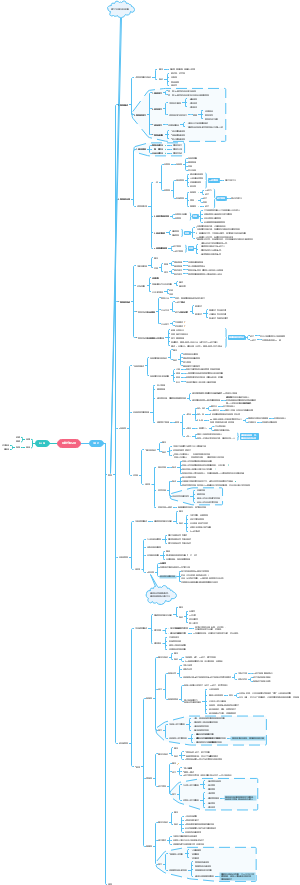
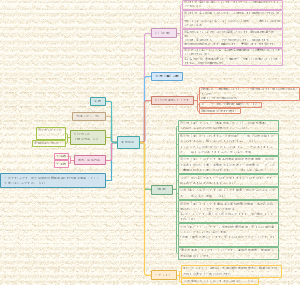
Immune system
I这是一篇关于mmune system的思维导图,对mmune system感兴趣的小伙伴可以收藏起来观看,希望对大家有所帮助。
编辑于2022-06-14 18:22:29- Immune s…
- Hematop…
- Adaptive …
- Cells
- phagocytes
- 相似推荐
- 大纲
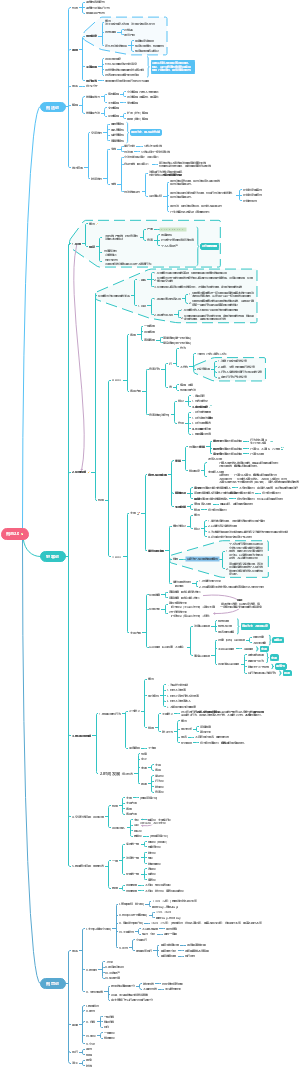

Immune system
Innate system
temperature
constantly 37, even higher under fever/inflammation
fatal to 40.6℃
39.4℃ is already really dangerous
Surface
tissues structure
close barrier
skin
mucous
small particles
antimicrobial peptides in secretory fluids
defencins
lungs & gastrointestinal tract
lysozyme
breaks down the cell wall of bacteria.
Lactoferrin and transferrin
By binding iron, an essential nutrient for bacteria, these proteins limit bacterial growth.
protones
acidic sweat, acidic gastric fluid
oils
salts
microorganisms
normal flora
inner anotomical structures
blood-brain barrier
blood-placental barrier
blood-thymus barrier
Proteins
PRRs(pathogen recognation receptors)
membrane
Toll-like receptors (TLRs)
The portal between Innate and adaptive systems
TLR1-TLR10
stimulates intracellular cascades
induce transcription factor NF-kβ
releases
IFNα, IFNβ
if viral finds
CD40, CD80, CD86
stimulates Tcell
Inflammation/fever involved ILs
IL1
only one induces fever
other chemokines attract phagocytic cells and T,B cells
here recruits also adaptive immune cells
often found in sentinal cells
Epithelial cells
Dendritic cells
Phagocytes
macrophages
neutrolphiles
binding pockets
repeated leucin rich region to binds PAMP
C3b receptors
On all phagocytes
binding to C3b oposonized pathogen surface
Mannose receptors
Cytoplasmic
NOD-like receptors
Rig-helicase like receptors
help responding to viral RNA
response after phagocytosis
Secreted
sereum oposonin
mediate phagocytosis recognation
ex. C3b
one domain binds to PAMP, another domain binds to oposonin receptors on phagocytes surface
lectin family
Mannose binding lectin(MBL) protein
binds mannose containing carbohydrates on bacteria
The binding splits C2 and C4 then activates complement system
each PRRs recognizes a particular PAMP
Mannose
peptidoglycan
lipopolysaccharide in gram negative bacteria
flagellin proteins
zymosan from yeast cell wall
unmethylated CPG motifs in bacterial DNA
viral DNA/RNA
inflammation complementing proteins
~30 different proteins normally circulating in blood
They can enter tissue during inflamation
activation in protease cleavage cascades
9 small protein precursors C1-9 normally circulating in blood
complex protease cascades
C5 convertase
classical C3 convertase
can be activated by
antigen binding IgG
further enhacing of Innate inflamation by adaptive system
classicle pathway
mannose binding lectin
side pathway
functional components after activation
C3a
activates phagocytes
induce vasodilation of endothelial cells in nearby blood vessels
C3b
oposonization
to facilitating phagocytosis by oposonin receptors on them
Chemokines attract macrophages and neutrophiles
also may through receptors of C3b on their surface
part of C5 convertase
C5a
activates phagocytes
especially neutrophiles
induce vasodilation of endothelial cells in nearby blood vessels
MAC
form pore on bacteria cause cell swell and burst
not effective for the pathogens who have outer lipid membrane
other results caused by complement proteins
stimulate mast cells and basophils to release histamine
further enlarge inflammation
Interferon
all cells can synthesis when viral infection
IFN-α
antiviral
IFN-β
antiviral
They induce neighboring cell death
by induce neighboring cells RNA degredation and blocks protein production
Only produced by T lymphpcytes and NK cells
IFN-γ
activates macrophage
immonological defense against infection and cancer
Cells
phagocytes
general process of phagocytosis
process(RAID)
Recognition
direction
by chemokines
C3b
macrophages "Fishing"
using long, sticky cytoplasmic extention
by surface receptors
oposonin receptors
like C3b receptors
TLRs
4 major receptors
TLRs
lgG FcR
CR
Scavenger R
Adherence
antigen and bacteria adhere to Macrophages membrane
Ingestion
Pseudopodia help ingestion, form phagosome
Digestion
defensin
only by neutrophiles
lysosome
intracellular using Reactive oxygen and nitrogen intermediates (ROI & RNI),
superoxide (O2-), hydrogen peroxide (H2O2), peroxynitrite (ONOO-).
fusion of it with endosome to form phagolysosome
discard
The indigestable materials form residual bodies and are discarded
neutrophiles(PMNs)
life cycle
short 1-2d
normally circulating in blood
50-70% peripheral blood leukocytes
number further increases when acute inflammation
role
most fast response cell type appear where the tissue damage/infection/ local inflammation
by squeezing through capillary endothlial cells
pus is a mixture pf dead pr dying pathogens, tissue cells, and neutrophils.
eat most pathogens
lysosome
with greater range of reactive oxygen radical than Macrophages
also includes defensin
signaling
secretion
cytokines
IL-1/2/4
fever!
chemokines
activate both innate and adaptive immunity.
Macrophages(Mψ)
Size
large, irregular shapped
life cycle
long, with regenerated lysosomes
monocytes roam continuously in extracellular fluid that bathes tissues
it's attracted to connective tissue when tissue injory, and mature there
by squeeze through capillary endothlial cells
It is usually slower, that follow the neutrophile
roles
eat most pathogens
extracellular killing infected cells
tissue repair
eat cellular debris leaved after apoptosis and dust in lungs
signaling
APC
activated by
IL2, IFγ
can be secreted by Th1
secretion
cytokines
IL-1/2/4
fever!
chemokines
activate both innate and adaptive immunity.
differenciate from Monocytes
Monocytes mature in infectious site
killer cells
Dendritic cells(DC)
Mast cells
Eosinophils
function
anti-parasites
kill way
proteins in its granue
NK cells
role
induce apoptosis in viral infected and malignent cells
molecular detail
Nk cell release perforins and granzymes
perforins first insert into membrane of target cell, and polymerize into a pore
granzymes enter the pore and activate caspases in target cells
activation of caspases induce apoptosis
Platelates
inflammation
Inflammatory response
syndrom
5 hall marks
Red
Warm
edema(tissue swelling)
pain
potential fuctional lost
can be locolized, systemic
can be acute, chronic
inflamatory trigger(mediator) proteins
red warm related signals
histamine
normally released in damaged cells
release can be stimulated by activated complement molecules
prostaglandins
normally released by damaged cell
bradykinin
effects
dilate the local blood vessels and then increase the local blood flow
also increase the vascular permeability
so allow complement proteins to get in tissue
Effects amplified by Complement proteins cleavages
can be activated by
pathogen on mannose binding lectin
pathogen binding IgG 's Fab region
Increase vascular permeability
let first-line neutrophiles path through
by C3a, C5a
activates phagocytes metabolism
C3a, C5a
Recruit neutrophiles(chemotaxis)
by C5a
Oposonization
by C3b
Cytolysis
by MAC
acute phase proteins
may not only complement proteins
1000folds when inflammation
stimulites phagocytosis
causing liver and spleen to store ion
Many bacteria need high blood ion level to grow
inflamatory enlargement through some leukocytes
Mast cells
Basophiles
also activated during allergic responce
inflamatory factors released cause allergy
both release inflamatory mediators
histidine
prostaglandin
both releasing is activated by cirtain activated complement proteins
They have IgE receptors on their surface
also activated by antigen cross linking of two variable regions of neighboring IgE
acute phase response: Fever
induced by IL-1
secreted by TLRs signaling
in all phagocytes
epithelial cells
DC
effector
neurons of hypothalamus in brain
increases body temperature
adaptive system
antigen
sources
components of a microorganism or virus.
proteins or glycoproteins on the surface of transfused RBCs or transplanted tissue
components of foods or pollens
epitopes
antigenic determinants
An antigen often contains more than 1 and 1 types of epitopes
ex. 1 protein can have 6 epitopes, each may stimulates a distinct immune response
epitope binding molecules
not germline encoded
generate by DNA-rearragement during maturation in primary lymphatic organ
antibody/Ig
questions
producing a lot of "fucosing" molecules
Why the targeting molecule can always cure the disease if it arise properly?
How can we design a targeting molecule for some pathogen that body never ever seen before?
by speeds up evolution
How can they know that what things should not in the body,but what things should?
so they should be selected!
Structure
4 subunits
2 heavy
determine Fc portion
2 light
Y shape
Variable region(Fab region)
2 tips of Y shape
110-130 aa
specificity
ends of both heavy and light chains
constant region(Fc portion)
the rest part
determines the mechanism used to destroy antigen.
Variations
IgG
monomer
no synthesis until birth
but maternal IgG can cross placenta
4 subclasses
70-75% total Ig
activates complement system
require 2 units
2 Fab region bined Fcγ region, activates C1 protease activaty
Fcγ can binds to all Fcγ receptors
Opsonization and phacilitates phagocytosis of microbes
all phagocytes have Fcγ receptors
Antibody-dependent cellular toxicity
NKs have Fcγ receptors
Eosinophils have Fcε receptors
major Ig in secondary immune response(memory B cells)
also very much in primary response, but a little slower than M
IgA
dimer
no synthesis until 1-2 months after birth
but high quantity in milks
Most abundant form of antibody in body secretions.
High density of IgA-secreting plasma cells in MALT
3 subclasses for 15%-20% total Ig
IgM
pentamer
only presents in intravescular pool
First antibody secreted during the primary immune response
secondary immune response also presents a little
promotes agglutination and precipitation reactions and activates complement
requires only one unit
10% total Ig
IgD
Monomer
Present only on surface of B cells; serves as antigen receptor
<1%
IgE
Fc region binds to mast and basophils
allergen binding to V regions promotes the release of mediators, which triger allergic reactions
allergern cross links variable regions of 2 neighboring IgEs
application
specific "probe" in technique
roles
Neutralization of microbe and toxins
Opsonization and phagocytosis of microbes
phagocytes have Fcγ receptors
Antibody-dependent cellular toxicity
NKs have Fcγ receptors
Eosinophils have Fcε receptors
Complement activation
MAC lysis
C3b opsonization
c3b receptors on phagocytes
other factors enhance inflammation
sequence during primary/secondary responses: 1: IgD-IgM 2: IgG-IgA-IgE
receptors
10^5 receptors per cell
BCR
binds to floating antigens
and B cell takes up that antigen and presents it on MHCII, waiting for Th cell activates clonal expansion
TCR
only binds to MHC bonded antigen presenting molecules
Antigen presenting
Antigen presenting cells: APC
professional APC
DCs, Macrophages, B cells
contains both MHC class I and II
may cross presentation
only group which can activates T helping cells
DCs
T cells clonol selection in thymus using most DCs MHC II as selective tool
DCs activates most Th cells
actually B cells and Macrophages are be activated by activated Th cell through MHC2-pathogen CD4 linkage
Macrophages
The MHCII on it is mostly let it self be activated
B cells
its surfacte MHCII activation is essential to activates B cells massive clonal expansion
nonprofessional APC
Glial cells, thymic epithelia cells
only contains MHC class I
actually all nucleuated cells
MHC classes
MHC class I
antigen presenting to CTL(CD8+ T cells)
together assisted by ligating CD8
MHC class II
antigen presenting to helper T cells (CD4+ Th cells)
together assisted by ligating CD4
process
endogenous MHC I pathway
1. proteosome digests intracellular viral proteins into antigen
2. the antigen path through ER into ER lumen
3. the antigen binds to the ER lumen bonded MHC class I within ER lumen
4. The antigen bonded MHC I is merged with cytoplasm through exocytosis
exogenous MHC II pathway
1. extracellular pathogen entered through phagocytosis
2. the pathogen is degested within phagosome
3. phagsome surface contain MHC II and bond to antigens within phagosome
4. the phagosome further merge with plasma membrane
Co-recepors: CD8 for Tc and CD4 for Th
Th activation also requires binding of CD28 and B7 on professional APC
ONLY BINDs Protein epitopes
Then presenting of those MHC results in
Clonal selection
with identical receptors/ antibody produced
Primary lymphoid tissues' Training process, an accelerated cellular evolution process
Location
Primary lymphoic tissue
T cells
thymus
B cell
bone marrow
results
90% B cells apoptosis
because they bind surface self antigen of to bone marrow stromal cell
95-98% T cells undergo apoptosis
They binds too tight to MHC- self peptite complex on Thymus Dendritic cell
or They don't bind to MHC at all
because CD8/4 should bond to MHC along
Clonal expansion
location
secondary lymphoic tissue
The pheriphral region is filled with antigen
The best way to let naive lymphocytes activated
They "luck one" will finally successfully catch the antigen, then it's get clonal expansion
results
generates effector cells
activated Th
activated Tc
effector B/plasma cells
produce identical Ig variable regions like the receptor
Activated Th involve in B cells activation
by using it TCR and CD4 binds to MHC-2 on B cell
Th releases IL-4, the preprequest for B cell activation
apoptosis after 14 days
generates memory cells
last forever
reactivated by next receptor activation
Destruction of infected nucleoated cells by Tc
Activated Tc binds MHC-1 antigen complex with CD8 assists
induce target cell apoptosis
Enhance function of macrophage
Activated Th binds to MHC-2 antigen complex with CD4 assists
Macrophage release IL-12
Th responces IFN-γ
Macrophage destroying function is enhanced
The time axis
0 day
1. Direct stimulation of naive B lymph cell
2. Antigen presenting to naive T lymph cells
0-7day
clonol expansion of lymph cells
4-day differentiation into
The route of focusing
questions
many "professional" cells help the focusing process
Some times the biggest problem is our self cells
so some cells must die
they are controled by viruses.
they accidently become mad!
Why we need other cells called CD4+cells?
kill non-self is done by CtT cells
secreting antibodies is by B cells
eating dangerous things is by macrophages
isn't it perfect?
Organs
central/primary lymphoid organs
thymus
Bone marrow
mature of progenitor B cells
Mature
where DNA rearrangement happends
B/T cells aquires specific receptors
and they followed by trainning processes
Clonal selection(the process of maturation)
Location
Primary lymphoic tissue
T cells
thymus
B cell
bone marrow
results
90% B cells apoptosis
because they bind surface self antigen of to bone marrow stromal cell
95-98% T cells undergo apoptosis
negative slelection
They don't bind to MHC at all
because CD8/4 should bond to MHC along
positive selection
They binds too tight to MHC- self peptite complex on Thymus Dendritic cell
with identical receptors/ antibody produced
Primary lymphoid tissues' Training process, an accelerated cellular evolution process
periphral/secondary lymphoid organs
lymph nodes, spleen
MALT
mucosa-associated lymphoid tissue. ex. small intestin
clonal expansion
Where antigen is collected, and stimulate mature/naive lymphatic cells' clonal expansion
Some tricky terms
Cytokines
extra cellular immunmodulating signaling proteins such as interleukin and interferion
cytokines
Interferon(IFN)
all cells can synthesis when viral infection
IFN-α
antiviral
IFN-β
antiviral
They induce neighboring cell death
by induce neighboring cells RNA degredation and blocks protein production
Only produced by T lymphpcytes and NK cells
IFN-γ
activates macrophage
immonological defense against infection and cancer
They also connect lymphocytes' prolyferation
Interleukine(IL)
complex signaling functions
trigure favor, inflammation, Tcells differenciation
IL-4
activates B cell clonal expansion
released by Th1 MHCII recognation
IL-12
enhance Macrophages phagocytosis
released by Th0 MHCII recognation
Chemokines
a family of small cytokines
they are common in inducing chemotaxis of cells
ex. Cb3 in complement system, attract neutrophiles and Macrophages, also C5a attracts neutrophiles
usually attracts phagocytes。。。
leukocytes
also called white blood cells (WBC)
circulating in body and nonspecifically attack pathogens within tissue
extracellular fluids
fluids that bath tissues
debris
The vesicles leaved after apoptosis
immune surveillance
The function of checking and eliminating malignent cells before they develope into a detectable turmor, like NK cells
always have a chance of failure/success
progeniter
mean by cells that are not mature
Mature
means lymphocytes have already aquired their surface antigen-binding receptors in primary lymphatic tissue
after the "training"?
Naive
means lymphocytes are mature, but the antigen-binding receptors are not activated and still not under go clonal expansion
Activated
means the activated, mature lymphocytes
Main Topic
hematopoitic stem cells
Hematopoisis
source of immune system
hematopoitic stem cells divide and differentiate into all cells found in blood
Innitially formed in yolk sac of embryo, then migrates to fetal liver and spleen finally to the bone marrow
Myeloid progenetor cells
phagocytes
phagocytosis
process(RAID)
Recognition
direction
by chemokines
C3b
macrophages "Fishing"
using long, sticky cytoplasmic extention
by surface receptors
oposonin receptors
like C3b receptors
TLRs
4 major receptors
TLRs
lgG FcR
CR
Scavenger R
Adherence
antigen and bacteria adhere to Macrophages membrane
Ingestion
Pseudopodia help ingestion, form phagosome
Digestion
defensin
only by neutrophiles
lysosome
intracellular using Reactive oxygen and nitrogen intermediates (ROI & RNI),
superoxide (O2-), hydrogen peroxide (H2O2), peroxynitrite (ONOO-).
neutrophiles have more species than phagocytes
fusion of it with endosome to form phagolysosome
discard
The indigestable materials form residual bodies and are discarded
neutrophiles(PMNs)
life cycle
short 1-2d
normally circulating in blood
50-70% peripheral blood leukocytes
number further increases when acute inflammation
role
most fast response cell type appear where the tissue damage/infection/ local inflammation
by squeezing through capillary endothlial cells
pus is a mixture of dead or dying pathogens, tissue cells, and neutrophils.
eat most pathogens
lysosome
with greater range of reactive oxygen radical than Macrophages
also includes defensin
signaling
secretion
cytokines
IL-1/2/4
fever!
chemokines
activate both innate and adaptive immunity.
Macrophages(Mψ)
Size
large, irregular shapped
life cycle
long, with regenerated lysosomes
monocytes roam continuously in extracellular fluid that bathes tissues
it's attracted to connective tissue when tissue injory, and mature there
by squeeze through capillary endothlial cells
It is usually slower, that follow the neutrophile
roles
first-line against most infections together with neutrophiles
a little slower than neutrophiles
link between innate and adaptive system
TRR
MHC II
extracellular killing infected cells
tissue repair
eat cellular debris leaved after apoptosis and dust in lungs
signaling
APC
activated by
IL-12, IFγ
can be secreted by Th1
must through MHC-II recognation
secretion
cytokines
IL-1/2/4
fever!
chemokines
activate both innate and adaptive immunity.
professional antigen presenting cells
MHC II
differenciate from Monocytes
monocytes normally circulating in blood
Monocytes mature in infectious site
receptors
CCR5
co-receptor CD4
that's why HIV can enter
first cellular line defence
other cells
Dendritic cells(DC)
activates T cells
link between Innate system and adaptive system
different TLRs regocnizes pathogens
secretes cytokines
trigre inflammation
Also the major Th cell activator
professional antigen presenting cells
MHC class II activates T helping cells
also contain MHC class I activates Tc cells
It's also the major T cell clonal selection responsible cells in thymus
inflamatory mediators releasing cells
Mast cells
can be activated by Th2
Basophiles
also activated during allergic responce
inflamatory factors released cause allergy
both release inflamatory mediators
histidine
prostaglandin
both releasing is activated by cirtain activated complement proteins
They have IgE receptors on their surface
also activated by antigen cross linking of two variable regions of neighboring IgE
Eosinophils
function
anti-parasites/eliminate helmines
kill way
proteins in its granue
perforins
form pores on helminth skin plasma membrane
degestive enzymes
ingect into perforin pores
exacerbate chronic inflammatory diseases
asthma
IBD
inflammatory bowel disease
Platelates
erythrocytes
only one that not involved in immunity
Lymfoid progenetor cells
T cells
Helper T cells
naive form activated most by DC MHCII bonded antigen
After that It's a dynamic differentiating form
h0>h1>h2
activates a lot of cells by releasing cytokines
Th0
Induction of cytotoxity in CD8+ CTLs.
Th1
recruits & activates macrophages
needs MHC II
Induce antibody isotype switching: increase IgG antibody.
Th2
activates B cells
needs MHC II
activates mast cells
inflammation
releases cytokines
Cytotoxic T cells
naive form activated by MHC I bonded antigen
by both professional/non professional APCs
kill "alter-self" cells
virually infected
tumor cells
TCR+CD8 Recognize infected cellular surface MHC I-antigen
Perforin-induced apopotosis
perforin+A&B Granzymes
Fas-mediated apoptosis:
Upregulate FasL via Fas-FasL
mature in thymus
B cells
have surface BCR, and can binds specific antigen
BCR is IgD
DO NOT need antigen presenting
BCR binding activates clonal expansion into
plasma cells
nolonger have surface BCRs
a biochemical factory devoted to the secretion of antibodies directed against specific antigens
memory B cells
professional antigen presenting cells
MHC II
but seems be activated by CD8+ cells
release IL-4 stimulates Naive B cell colonal expantion
mature in bone marrow
NK cells
role
Fast induce apoptosis in viral infected and malignent cells
molecular detail
Nk cell release perforins and granzymes
perforins first insert into membrane of target cell, and polymerize into a pore
granzymes enter the pore and activate caspases in target cells
activation of caspases induce apoptosis
can release IFN-γ
The real pathway of their differentiation