导图社区 先心病各论
先心病各论
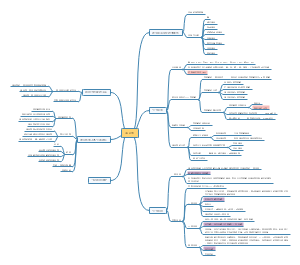
先心病各论,分享了 室间隔缺损 VSD、动脉导管未闭PDA、房间隔缺损ASD、法洛四联症TOF的知识,一起来看看。
编辑于2023-04-12 23:37:56 上海他的近期作品
查看更多>>
- 肝肿瘤
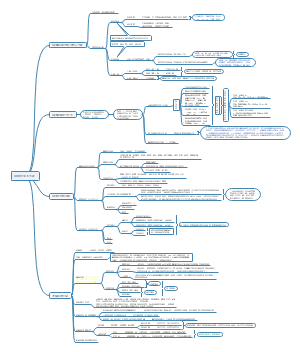
肝肿瘤思维导图,分为肝恶性肿瘤、转移性肝癌 Metastatic Liver Cancer、肝良性肿瘤的知识,快来看。
- 染色体畸变 _Chromosomal Aberrations_遗传代谢病_Inborn Errors of Metabolis,IEM
染色体畸变 _Chromosomal Aberrations_遗传代谢病_Inborn Errors of Metabolis,IEM,一起来看。
- 胰腺癌及壶腹周围癌
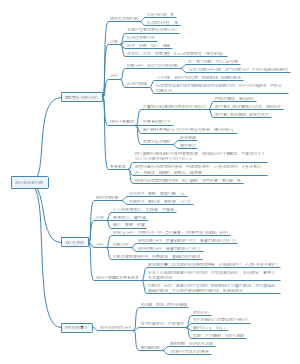
胰腺癌及壶腹周围癌,需要掌握: 胰腺癌及壶腹周围癌的临床表现、诊断要点及治疗原则。 熟悉:胰腺癌及壶腹周围癌的治疗方式。 了解:胰腺癌及壶腹周围癌的病因、发病机制以及病理生理。
先心病各论
社区模板帮助中心,点此进入>>
他的近期作品
查看更多>>
- 肝肿瘤
肝肿瘤思维导图,分为肝恶性肿瘤、转移性肝癌 Metastatic Liver Cancer、肝良性肿瘤的知识,快来看。
- 染色体畸变 _Chromosomal Aberrations_遗传代谢病_Inborn Errors of Metabolis,IEM
染色体畸变 _Chromosomal Aberrations_遗传代谢病_Inborn Errors of Metabolis,IEM,一起来看。
- 胰腺癌及壶腹周围癌
胰腺癌及壶腹周围癌,需要掌握: 胰腺癌及壶腹周围癌的临床表现、诊断要点及治疗原则。 熟悉:胰腺癌及壶腹周围癌的治疗方式。 了解:胰腺癌及壶腹周围癌的病因、发病机制以及病理生理。
- 相似推荐
- 大纲