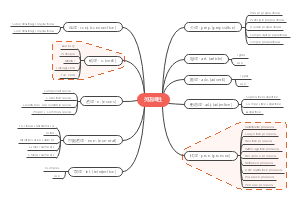
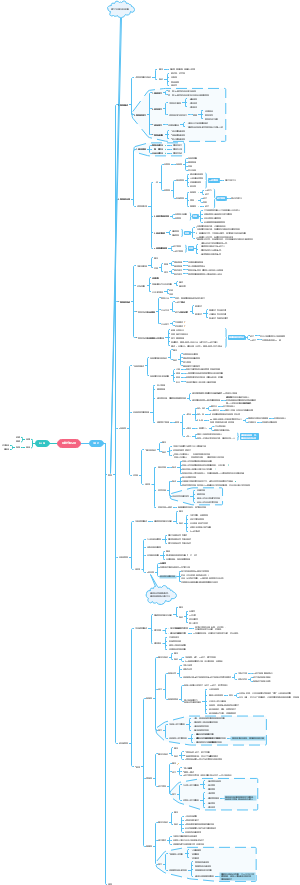
导图社区 acid and alkali
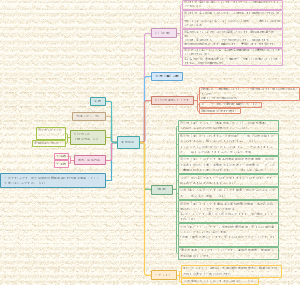
关于泌尿系统病生酸碱平衡的思维导图,主要内容有acid、alkali、material resourse、Butter system in body等。
社区模板帮助中心,点此进入>>
英语词性
法理
刑法总则
【华政插班生】文学常识-先秦
【华政插班生】文学常识-秦汉
文学常识:魏晋南北朝
【华政插班生】文学常识-隋唐五代
【华政插班生】文学常识-两宋
民法分论
日语高考動詞の活用
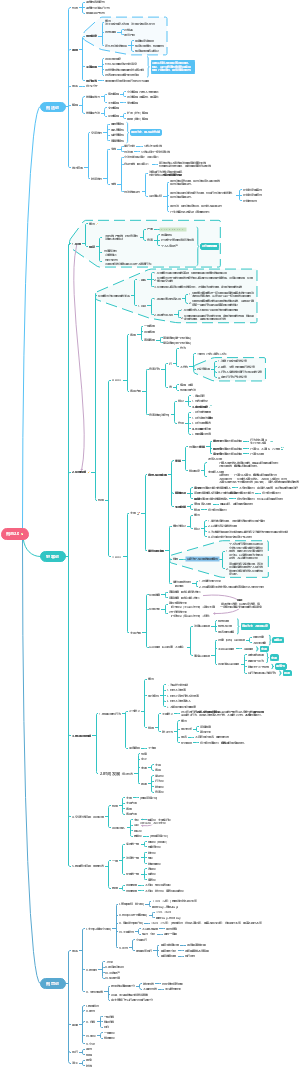
acid and alkali
acid
Volatile acid
H2CO3
Fixed acid(unvolatile acid)
medicine
氯化铵(ammonium chloride)、水杨酸(salicylic acid)
磷酸(phosphoric acid)、乳酸(lactic acid)、尿酸(uric acid)、酮体(ketone body)、三羧酸(tricarboxylic acid)、硫酸(sulphuric acid)
alkali
material resourse
mainly from food intake
mainly from the body
entirety
acid drainage and alkali retention
Butter system in body
blood buffering system
bicarbonate /carbonic acid
features
1.strongest capacity(55%)
2.open regulation available throngh kidney and lungs
3.can buffer all unvolatile acid,haven't capacity to buffer volatile acid
4.The blood's pH is decided by the ratio of H2CO3 and HCO3-
the regulation of lungs
regulate the ratio of carbonic acid through the regulation of the emiton of carbon dioxide(volatile acid)
centrol control
PaCO2
normal value
40mmHg△2mmolHg
60mmHg---10 times
>80mmHg---carbondioxide narcosis---inhibitory effect
peripheral control
cell regulation
mainly through the exchange of ion in and out of cell
acidosis
hyperkalemia (高血钾)
alkalosis
hypokalemia (低血钾)
renal regulation
excrete fixed acid
maintian the value of carbon dioxide in plasma
H+secretion and NaHCO3 reabsorption in proximal renal tubules
exchange of Na+ and H+
the activity of CA(carbonic anhydrase)
can catalyze the cobination of H2O and CO2 to H2CO3 then dissociate toH+ and HCO3-
urine acidification is not obvious
H+secretion and NaHCO3 reabsorption in distal renal tubules and collecting ducts
H+---ATP
CA activity
urine acidification is obvious
Excretion of NH4+(severe acidosis)
Proximal convoluted tubules:
Glutaminase(谷氨酰胺酶) activity
Na+- NH4+exchange
Distant curved tubules and manifolds:
When pH<4.8, secrete NH3 to neutralize H+
Secretion of H+, NH4+and reabsorption of HCO3-
laboratory parameters of acid-base disturbance
pH
normal value 7.35·7.45
PH < 7.35 decompensated acidosis
PH > 7.45 decompensated alkalosis
• Normal acid-base balance
• Compensatory acid-base poisoning
• Acid and alkali poisoning co-exist and mutually offset
Inversely proportional to alveolar ventilation与肺泡通气量成反比
Respiratory factors呼吸性因素
PaCO2 < 33mmHg pulmonary hyperventilation, found in primary respiratory alkali or compensatory acid
PaCO2 > 46mmHg pulmonary hypoventilation, seen in primary respiratory acid or compensated offspring alkali
SB、AB
代谢性因素 呼吸性因素
Normal value: 22~27 mmol/L (average 24 mmol/L)
Normal person AB=SB
AB=SB < 22 mmol/L, found in primary acid
AB=SB>27 mmol/L can be seen in primary alkali
Respiratory factors of difference between AB and SB
If SB is normal, AB>SB, it indicates CO2 retention, which is found in primary expiratory acid
If SB is normal, AB < SB, it indicates that CO is discharged too much, which can be seen in the primary respiratory alkali
buffer base, BB
Concept: the sum of all negative ion bases with buffering effect in the blood.
Metabolic factor
Normal value: 45~52mmol/L (average 48 mmol/L)
BB < 45 mmol/L can be seen in primary acid
BB > 52 mmol/L can be seen in primary alkali
Normal value: - 3.0~+3.0 mmol/L
The increase of negative BB value indicates that the alkali is insufficient in the primary generation of acid
The increase of positive BB value indicates that the excess alkali is found in the primary generation of alkali
6.Aniongap,AG
UA(+)-UC(-)
normal value10-14mmol/L
meaning
Reflect the content of plasma fixed acid
Distinguish the acid type (AG > 16 mmol/L,which tips the metabolic acidosis)
Diagnosis of mixed acid-base balance disorder
summary
metabolic
AB,SB,BB,BE
repiratory
AB-SB,PaCO2
AG
type of (metabolic) acidosis (>16mmol/L)
Classification of acid-base disorders
Compensability
Decompensatory
Compensatory
type
simple
metabolic acidosis
PH decrease caused by increase of fixed acid and/or loss of HCO3 -
Characteristics: Primary decrease of plasma HCO3-
Causes and mechanisms
Acidosis
Increased production of fixed acid
Lactic(乳酸) acidosis: shock, heart failure
Ketoacidosis(酮症酸中毒): diabetes(糖尿病), severe hunger, alcoholism
Reduced acid excretion
Severe renal failure
Type I RTA (renal tubular acidosis)
----Distal convoluted tubular(远曲小管) acidosis
Dysfunction of H+secretion
Urine cannot be acidified H+accumulation
Excessive intake of exogenous fixed acid
Hyperkalemia
Alkalosis
HCO3 - excessive direct loss
Severe diarrhea(严重腹泻), small intestine (肠道萎管) and biliary tract atrophy(胆道萎管), etc
HCO3 - reduction of absorption
Type II RTA: proximal convoluted tubule(近曲小管) acidosis
Application of carbonic anhydrase (CA) inhibitor (reduce the formation of H2CO3, the secretion of H+, and the reabsorption of HCO3 -)
Hemodilution HCO3 decrease
A large amount of sugar water or salt water is input in a short time
classification
AG increased metabolic acidosis"Normal blood chlorine(氯) metabolic acidosis"
AG increased (fixed acid increased)
Normal blood chlorine
cause
Fixed acid retention
Lactic acidosis
ketoacidosis
Poisoning by salicylic acid(水杨酸)
Phosphoric acid(磷酸) and sulfuric(硫酸) acid excretion disorder
Normal AG metabolic acidosis"Hyperchloric metabolic acidosis"
AG is normal
Increased blood chlorine
causes
Alkali deficiency
diarrhea(腹泻)
Hyperkalemia(高钾血症)
Renal tubular acidosis(肾小管性酸中毒)
A large amount of normal saline(生理盐水)
Excessive input of chloric acid salt(含氯酸性盐摄入过多)
mixed